Flexible endoscopy encompasses a large variety of heat sensitive, complex and intensively used medical devices with high risk for patients.
Flexible endoscopes may be critical or semi-critical according to Spaulding classification:
- Flexible endoscopes such as ureteroscopes, cystoscopes, hysteroscopes, or choledoscopes enter sterile cavities and are critical devices deserving terminal low temperature sterilization (LTS). By default, If manufacturer instructions for reprocessing do not propose any LTS option or if the recommended LTS cycles are not available to the hospital, the critical flexible endoscope may be disinfected with a chemistry effective on all germs including spores (see cleaning and disinfection) before final rinsing with sterile water.
- Gastro-intestinal (GI) and respiratory flexible endoscopes that come into contact with intact mucous membranes are semi-critical and candidates for high-level disinfection (i.e. a chemistry with partial effectiveness on spore – see cleaning and disinfection)
- Flexible endoscopes used for procedures such as endoscopic retrograde cholangiopancreatography (ERCP), interventional endoscopic ultrasound (EUS), endobronchial ultrasonography (EBUS), or for obtaining biopsy specimen are most often high-level disinfected, although they involve accessories which cross the mucous membrane. These endoscopes also include channels which are difficult to clean; for example, the forcept lift channel (also known as elevator channel) of duodenoscopes,
When the Spaulding classification was proposed, procedures such as ERCP, EUS, and EBUS did not exist. A consensus exists to consider the surgical accessories that cross the mucous membrane as critical items that must be single use or sterilized but opinions diverge on whether the endoscope itself is also of critical nature. Such hesitancy must not slow down the adoption of reprocessing methods that offer a higher margin of safety for patients. Positioning those endoscopes as critical devices will encourage progress.
Reprocessing of flexible endoscopes
For flexible endoscopes, the first reprocessing step, known as bedside cleaning, takes place at point of use.
The subsequent reprocessing steps are performed in a reprocessing room located close to the point of use, or are centralized under the responsibility of the sterilization department. In all cases, reprocessing is performed by trained operators dedicated to these tasks.

Centralized reprocessing of flexible endoscopes benefits from the skills and quality management system of the sterilization department. Drawbacks of centralization are of logistic nature, in particular when the sterilization department is at distance from the point of use. This may result in slowed turnover that may have to be supplemented by acquiring a higher number of flexible endosocopes.
Sterilization of flexible endoscopes is performed after point of use processing (bed-side cleaning), pre-cleaning, cleaning, drying, and packaging and is followed by storage in a sterile barrier system until use.
High-level disinfection of flexible endoscopes includes: point of use processing, (bed-side cleaning), pre-cleaning, cleaning, intermediate rinsing, high-level disinfection, final rinsing, drying, and storage.
Point of use reprocessing (bed-side cleaning) and pre-cleaning are manual. Cleaning, intermediate rinsing, disinfection and final rinsing are manual or automated (preferred).
Manual cleaning and disinfection
Endoscopes are completely immersed in baths. Ideally, distinct sinks are used for each step (precleaning, cleaning, intermediary rinsing, disinfection, and final rinsing with filtered water).
Baths are prepared in large sinks that allow operators to stretch the endosocope and minimize the risk of damage during channel brushing (see below). Manual cleaning workstations may be equipped with pumps that deliver a defined flow of detergent or disinfectant solution in endoscope channels.
Disinfectant baths are preferably single use. When they are reused, the maximum number of reuses is defined by the disinfectant manufacturer. Indicators are used to control that the solution is above the minimum effective concentration.
Automated cleaning and disinfection
Automated endoscope reprocessors (AER) automatically adjust the dosage and temperature of solution and duration of each phase (cleaning, intermediate rinsing, disinfection, final rinsing with filtered water, air purge). In most cases drying is performed or completed manually.
Endoscope channels are connected to the AER and irrigated at predefined flow. Outer surfaces of endoscopes are sprayed and/or immersed.
Various types of AERs are available on the market. The more sophisticated can detect leaks, channel obstruction, disconnection of connectors and allow for reprocessing of all endoscopes including duodenoscopes.
Some AERs have pass-through configurations that separate the dirty and clean areas.
The AER must be periodically self-disinfected to prevent development of biofilm in distribution circuit. Self-disinfection is preferably thermal.
Final rinsing filter must be replaced according to AER manufacturer instructions or applicable guidelines. Failure of self-disinfection and final filtering remain among the most frequent sources of endoscope contamination.
AERs are sophisticated electronic and mechanical equipments subject to intensive use. Maintenance contracts and manual back up procedure must be organized to ensure process continuity.

Compliance of washer-reprocessor to international standard ISO 15883-4 is recommended and may be required in some countries
Maximum storage times before use or reprocessing are commonly defined by local regulations. In some countries, storage limits can be extended when endoscopes are placed in a storage cabinet that dries endoscopes, including lumens with filtered air, or confines them in conditions (e.g. vacuum) that prevent growth of germs.
Compliance of storage cabinet to international standard EN 16442 is recommended and may be required in some countries
Given the large variety of endoscopes, reprocessing equipment, chemicals, cleaning accessories, as well as guidelines and regulations applicable to flexible endoscopy, it is difficult to describe all reprocessing variants in detail. However, key principles can be summarized as follows:
All reprocessing operations take into account instructions for reprocessing of flexible endoscope manufacturer, sterilization, high-level disinfection equipment manufacturer, and chemistry manufacturers and are performed by trained operators. Endoscope accessories (e.g. valves) are reprocessed according to endoscope manufacturer instructions (preferably sterilized when possible).
- Point of use processing (bed side cleaning) is done immediately after use before bioburden has an opportunity to dry. The objective is to eliminate visible soils by wiping external surfaces and aspiration and flushing of lumens with large volumes of water and detergent. Operators’ hands are protected by single use gloves which are disposed of after the procedure.
- Transfer to the reprocessing room is done before remaining soil has an opportunity to dry. Soiled endoscopes are contained in a manner that prevent exposure of staff, patients, or the environment to potentially infectious organisms. An open container can suffice for transport to immediately adjacent reprocessing rooms, but fully enclosed containers or bags are required for transportation on longer distances. The container carries visible and clear indication that the flexible endoscope is contaminated.
- Leak test takes place before any immersion after removal of distal cap and valve). Leak test checks the integrity of the endoscope’s outer sheath. Leak test equipment and pressure are according to flexible endoscopes manufacturer’s instruction for reprocessing. If a leak is detected, the endoscope is sent for repair. The case or container used for transport to the maintenance workshop is agreed with the service provider and carries a visible indication that content is soiled.
- Pre-cleaning occurs within a defined time frame after use to avoid drying of soils and formation of biofilms. The endoscope is completely immersed in a detergent bath. All channels must be filled with cleaning liquid. Lumens are brushed with single use (preferred) or reusable brushes that were previously sterilized or high-level disinfected. The brushing direction depends on the endoscope type and manufacturer. External surfaces including valves, channels, connectors, and detachable parts of the endoscope are cleaned with soft cloth, sponge, or brushes. Valves are repeatedly actuated during cleaning to facilitate access to all surfaces. Brushes’ characteristics are according to flexible endoscope manufacturer instructions; in particular, those used for channels are adapted to the internal diameter for efficacy of cleaning and to avoid damage to the lumen.
- Point of use processing (bed side cleaning) is done immediately after use before bioburden has an opportunity to dry. The objective is to eliminate visible soils by wiping external surfaces and aspiration and flushing of lumens with large volumes of water and detergent. Operators’ hands are protected by single use gloves which are disposed of after the procedure.
- Transfer to the reprocessing room is done before remaining soil has an opportunity to dry. Soiled endoscopes are contained in a manner that prevent exposure of staff, patients, or the environment to potentially infectious organisms. An open container can suffice for transport to immediately adjacent reprocessing rooms, but fully enclosed containers or bags are required for transportation on longer distances. The container carries visible and clear indication that the flexible endoscope is contaminated.
- Leak test takes place before any immersion after removal of distal cap and valve). Leak test checks the integrity of the endoscope’s outer sheath. Leak test equipment and pressure are according to flexible endoscopes manufacturer’s instruction for reprocessing. If a leak is detected, the endoscope is sent for repair. The case or container used for transport to the maintenance workshop is agreed with the service provider and carries a visible indication that content is soiled.
- Pre-cleaning occurs within a defined time frame after use to avoid drying of soils and formation of biofilms. The endoscope is completely immersed in a detergent bath. All channels must be filled with cleaning liquid. Lumens are brushed with single use (preferred) or reusable brushes that were previously sterilized or high-level disinfected. The brushing direction depends on the endoscope type and manufacturer. External surfaces including valves, channels, connectors, and detachable parts of the endoscope are cleaned with soft cloth, sponge, or brushes. Valves are repeatedly actuated during cleaning to facilitate access to all surfaces. Brushes’ characteristics are according to flexible endoscope manufacturer instructions; in particular, those used for channels are adapted to the internal diameter for efficacy of cleaning and to avoid damage to the lumen.
- For Manual Cleaning the endoscope is placed in a detergent bath. Endoscope channels are flushed and the endoscope is maintained immersed according to manufacturer’s instructions. For automated cleaning, scope is installed in basin with gloves.
- For automated cleaning and disinfection, flexible endoscopes are then placed in AER basin with gloves. Lumens are connected as instructed, and the appropriate program is selected. It must be ensured that the endoscope and endoscope components can be reprocessed in the AER (e.g., the elevator wire channel of duodenoscopes is not effectively disinfected by most AERs, and this step should be performed manually). The next steps (intermediate rinsing (optional), disinfection, final rinsing, air purge, and in some cases partial drying) are performed automatically without additional operator intervention. In case of cycle failure, procedure is as instructed by the AER manufacturer. At the end of the cycle, operators control that both ends of channel connectors remain fitted to the endoscope and to the AER.
- Intermediate rinsing is performed with potable water at least. The objective is to eliminate detergent residues to avoid interaction with disinfection chemistries. Channel are irrigated and purged with air.
- Flexible endoscopes intended for low temperature sterilization are carefully dried with medical air or in a drying cabinet before packaging, sterilization and sterile storage until use.
- Disinfection achieves the targeted germ inactivation objectives (sporicidal in some cases). Immersion and channel irrigation times are according to chemistry manufacturer instructions. Channels are purged. If the disinfection solution is reused, routine controls (daily or more frequently in accordance with manufacturer’s guidelines) ensure at least the minimum effective concentration (MEC) of the active ingredient. If the chemical indicator shows that the concentration is less than the MEC, the solution is discarded.
- Final rinsing eliminates disinfection chemistry residues with filtered or sterile water. Channels are flushed. Connectors are reprocessed according to manufacturer recommendations, preferably sterilized. The rinse water is discarded after each use/cycle.
- Automatically reprocessed flexible endoscopes are withdrawn from the AER at this stage. See below information on isopropyl alcohol and drying.
- Drying eliminates rinsing water before storage. Outer surfaces and channels are flushed, preferably with medical air. When compressed air blow guns are used, it is recommended that they be removable and reprocessable (cleaning, disinfection and preferably sterilization). If contamination is found during regular microbiological testing of endoscopes, compressed air blow guns must also be included in the investigations and undergo microbiological testing.
In some countries there are recommendations to flush channels with with 70% to 90% ethyl or isopropyl alcohol to accelerate drying. This practice is prohibited in other regions due to the protein fixative properties of isopropyl alcohol.
- Sterilized endoscopes are withdrawn from sterilizer chamber. Time to availabity for reuse on patient depends on the low temperature sterilization method.
- Transfer to the storage zone is done in a manner that prevents contamination and damage of endoscopes. For long distance transfer, disinfected endoscopes are contained in a closed container or bag with visible indication that the content is disinfected. Transfer to an adjacent storage space or drying cabinet is performed with precaution to avoid any contact with potentially contaminated objects. Sterilized endoscopes are protected by a sterile barrier system. The packaging system is defined by risk analysis (see packaging).
- Storage rules for disinfected flexible endoscope vary according to applicable guidelines or regulation from a few hours to several days. In countries where rules do not allow overnight storage, the endoscope must be reprocessed before next use. The storage period may be prolonged by using storage cabinet.
Critical endoscopes that were disinfected must be used immediately after reprocessing. Sterilized endoscopes are stored in specified conditions and area. Maximum storage duration is event related and defined by risk analysis (see storage). Endoscope accessories are stored with endoscopes for traceability.
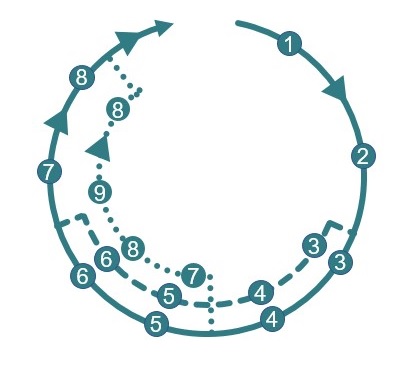
The above can be illustrated as below:
Storage of disinfected endoscopes in secure cabinets (preferably storage cabinets that prevent germ growth) Maximum storage duration is according to applicable guidelines.
9 Storage of sterilized, packaged endoscopes in a room dedicated to sterile items.
▲ Transfer of sterilized and disinfected endoscopes before or after storage is adapted to distance and risks.
10 Low temperature sterilization.
9 Packaging in Sterile Barrier system.
8 Drying with medical air to eliminates residual humidity that would favors germs growth.
7 Final rinsing with filtered water and air purge in AEWR. Sterile water for critical scopes (manual).
6 High-level disinfection of outer surfaces and channels. Sporicidal disinfectant for critical endoscopes.

Manual Reprocessing in sinks. Syringes or pumps for irrigation of channels

Automated Endoscope Reprocessor (AER)

Low Temperature Sterilization (LTS)
1 Point of use processing (bed-side cleaning) Immediately after use, outer surfaces are wiped channels are flushed.
▼ Transfer to reprocessing area in containers (closed if reprocessing room is not immediately adjacent). Indication of soiled content is visible.
2 Leak Test according to manufacturer instructions.
3 Pre-cleaning in a sink filled with a detergent solution. Endoscope, including channels is completely immersed. Soils are removed from outer surfaces and channels with adequate brushes. Channels are irrigated.
4 Cleaning (mechanical and chemical) with a detergent solution. Channels are irrigated during defined time. For non lumen endoscopes, cleaning may be combined with pre-cleaning.
5 Intermediate rinsing with at least potable water to remove cleaning residues and avoid interaction between cleaning and disinfection chemistries.
Endoscope reprocessing and quality management
Endoscope reprocessing processes are defined, validated and implemented in accordance with quality management principles.
Updated Standard operation procedures (SOP) are available.
Endoscope reprocessing undergoes process validation. An example of process validation for an automated endoscope reprocessors complying to ISO 15 883-4 is provided below. Validation of manual reprocessing can be adapted by withdrawing the tests which are not applicable. For validation of sterilization processes see process validation.
Show More
| Validation of automated thermal washer-disinfector processAccording to ISO 15883 |
IQ |
OQ |
PQ |
rQ |
RoutinePeriodic |
| Documentary verification |
P |
|
|
P |
|
| Verification of installation conformity
a. If the equipment was moved or connection to services was modified |
P |
|
|
Pa |
|
Cleaning efficacy on the cleaning stage alone on a surrogate device contaminated with artificial soil and on endoscopes contaminated by real use and representative of each family that can be reprocessed by the AER. Test soils, quantitative method, action and alert levels for OQ, and PQ according to ISO 15883-5 (2021). Part of PQ and OQ may be repeated at predefined periodicity (for example quarterly).
a. OQ: Test soils on walls of the chamber, carriers and load and 1 surrogate device selected according to annex H
b. PQ: After successful (a) endoscope contaminated by clinical use, control according to ISO 15883-5 on a scope representative of each endoscope type test group or family with the same connectors to the AER according to annex I of ISO 15883-4
| Channels |
Type test
group 1 |
Type test
group 1 |
Type test
group 1 |
| No channel |
|
|
P |
| Air/water |
P |
P |
|
| Biopsy suction |
P |
P |
|
| Instrument |
w or w/o |
|
Up to 2 |
| Water jet |
w or w/o |
|
|
| Elevator wire |
|
w or w/o |
|
| Control for balloon |
|
Up to 2 |
|
Type test group 1: Gastroscope and colonoscope, duodensocope with encapsulated elevator wire
Type test group 2: Duodenoscope with open elevator channel, endoscopic ultrasound, enteroscope
Type test group 3: Bronchoscopy, ear/nose, gynaecology and urology
c. Identical to initial OQ
d. Quarterly identical to b |
|
Pa |
Pb |
Pc |
Pd |
| Disinfection of liquid transport system after self disinfection cycle. Control of final rinse water after self-disinfection cycle (microbial count is less than 10 CFU/100 ml and absence of Pseudomonas aeruginosa in 100 ml) |
|
P |
|
|
P |
Leak test failure alarm
a. Quarterly |
|
P |
|
P |
P a |
Leak test non connection test
b. Quarterly |
|
|
P |
P |
Pa |
| Chamber leak proof |
|
P |
|
P |
|
| Door interlock |
|
P |
|
P |
|
Complete process
a. Control of process parameters through the whole cycle
b. Microbial control after real use on endoscope representive of each type test group according to Annex I of ISO 15883-4. Contaminated surrogate device when reguired by applicable guidelines.
c. Requalification is identical to initial OQ and PQ
d. Quarterly controls |
|
Pa |
Pb |
Pc |
Pd |
| Chemical dosing |
|
P |
|
P |
|
Water quality
a. optional |
|
P |
|
P |
Pa |
Air quality
a. optional |
|
P |
|
P |
Pa |
Drying with Anydrous copper sulfate paper
a. At frequency to be defined by user |
|
|
P |
|
Pa |
| Process residuals |
|
|
P |
P |
|
| Load carrier and trolley (fitting, force to move, alignment) |
|
|
P |
P |
|
Occupational health & safety measures are in place (in particular exposure to liquid and vaporized chemicals, aerosols and injuries by potentially contaminated RMD)
Protection of operators is adapted to the task being performed. In particular for manual pre-cleaning and cleaning body and face are protected from splashes or contaminants and chemical splashes by gloves, waterproof smocks with long sleeves, surgical mouth/nose masks, and eye protection. Particular attention is paid to ergonomics of workstation and muskoskeletal impacts of repetitive gestures. Eyewash stations are available to reprocessing staff using caustic chemicals.
Reprocessing fluids are discarded according to local waste management rules.
Facilities where endoscopes are used and disinfected provide a safe environment for to healthcare workers and patients. Air exchange equipment is used to minimize the exposure of all persons to potentially toxic vapors (e.g., glutaraldehyde). The vapor concentration of the chemical disinfectant used must not exceed allowable limits.
Training on SOP, routine controls, occupational health & safety and waste management take place and knowledge is periodically controlled.
A good understanding of various flexible endoscope configurations is essential. Training may be provided by endoscope and/or AER manufacturer, as needed. Competency testing of personnel is performed and documented on a regular basis (e.g., commencement of use, at least annually, any time a breach is identified, when a major technique or new endoscope or reprocessing equipment is introduced). Training and competency testing should include recognition of excessive wear or damage to instruments.
Maintenance plans are in place for dosing pumps, AER and sterilizers.
Traceability is operational.
Recommendation of WFHSS for the reprocessing of flexible endoscopes
- Flexible endoscope reprocessing is performed according to manufacturer instructions and in accordance with applicable guidelines
- Flexible endoscopes such as ureteroscopes, cystoscopes, hysteroscopes, choledoscopes are critical devices that should be sterilized. By default sporicidal disinfection with sterile water is applied.
- Semi-critical endoscopes are high-level disinfected,
- Flexible endoscopes used with accessories that cross the mucous membrane should be considered critical devices. Special attention is given to cleaning of complex endoscopes such as endosco ERCP, EUS and EBUS.
- Preparation of high-level disinfection or sterilization (i.e. point of use processing, pre-cleaning, cleaning) is performed with care according to detailed standard operating procedures. Complex flexible endoscopes with multiple and long channels such as duodenoscopes deserve special attention. Cleaning and high-level disinfection are preferably performed in automated endoscope reprocessors (AER).
- Operators are adequately trained and protected. Facilities and workstations are optimized to limit exposure to chemicals and minimize musculoskeletal impacts. Processes (manual or automated) undergo process validation.
↑